If you need to print this PDF or save for later
click below to download your copy.
[button size=”medium” style=”secondary” text=”Download PDF” link=”https://vetovationnew.instawp.xyz/wp-content/uploads/2016/01/Laparoscopy-article-10-18-15-Dr.-Case1.pdf” target=”none”]
MINIMALLY INVASIVE SURGERY: WHY IT’S NOT GOING AWAY AND WHAT IT MEANS TO YOU
J. Brad Case, DVM, MS, DACVS College of Veterinary Medicine University of Florida, Gainesville, FL
OVERVIEW
Minimally Invasive Surgery (MIS) is defined as any surgery that results in less tissue trauma or pain when compared with a traditional “larger” approach. Minimally invasive surgery is sometimes referred to as “keyhole surgery” to reflect the small incision(s) that are used.
Because MIS is relative, the philosophy can be applied to many, if not all, surgical procedures so long as there is a comparison in which one technique induces more trauma than the other. For example, open reduction and rigid plate fixation for appendicular fractures is now being performed routinely in a minimally invasive fashion in certain cases. The difference between a traditional approach and a minimally invasive approach has to do with the length of the required skin incision and the degree of manipulation and disruption of the fracture segments. This minimally invasive approach to fracture repair is referred to as minimally invasive plate osteosynthesis (MIPO) and often requires intraoperative imaging (i.e., fluoroscopy) to guide the procedure. Similar procedures are being performed in veterinary neurologic surgery including spinal fracture reduction and fixation, intervertebral disk fenestration, and hemilaminectomy. These procedures are performed via small incisions under the guidance of intraoperative fluoroscopy and/or endoscopic cameras.
Veterinary laparoscopy is a form of MIS and is further defined as surgery of the peritoneal cavity using a video-telescope and small instruments, which are manipulated from the outside of the abdomen. Similarly, thoracoscopy or video-assisted thoracic surgery (VATS) is MIS within the thoracic cavity. Both laparoscopy and VATS require significant working space within the abdomen or chest, respectively, and require insufflation with carbon dioxide gas (laparoscopy) or pneumothorax (VATS) in most cases. These procedures are minimally invasive in that they require only small (typically 5‒20 mm) incisions to complete the procedure, which is in contrast to a traditional, much larger laparotomy or thoracotomy.
The list of laparoscopic and VATS procedures being performed in veterinary surgery is extensive and is continuously evolving as surgeons gain more experience and as technology facilitates development of newer procedures. For example, the introduction of bipolar energy-based vessel/tissue sealing and dividing technology has facilitated an explosion of new applications in both laparoscopic and VATS surgery, including ovariectomy, ovariohysterectomy, cryptorchiectomy, splenectomy, ureteronephrectomy, adrenalectomy, cholecystectomy, pericardectomy, peripheral lung lobectomy, and cranial mediastinal mass resection. Precision manufacturing of surgical implants has also facilitated the advancement of endoscopic and intravascular minimally invasive procedures: for example, tracheal stent placement for tracheal collapse, percutaneous coil embolization of intrahepatic portosystemic shunts, bland embolization and chemoembolization of visceral tumors, glue and coil embolization of vascular malformations and palliative stenting for malignant obstructions, to name a few. The combination of advances in imaging technology and high precision implant manufacturing has led to the development of a new discipline in both human and veterinary surgery, namely interventional radiology. Now, procedures that once required an open thorax and/or abdomen and risky vascular surgery are performed completely via an introducer through a peripheral artery or vein.
This shift to minimal surgical approaches has and will continue to occur in veterinary surgery just as it has in human medicine. For example, over the past 15 to 20 years, laparoscopic cholecystectomy has become the gold standard for the most common abdominal procedure performed in humans. Now days, if a medical doctor offers open cholecystectomy for elective cases, it is recommended that the patient get a second opinion, to put it kindly.
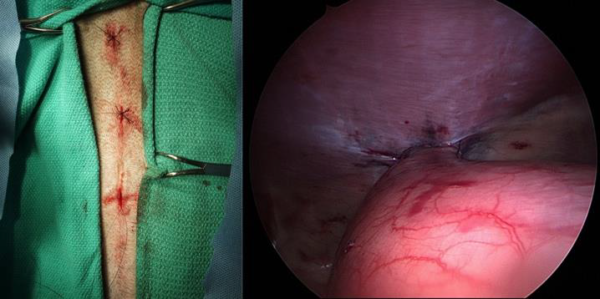
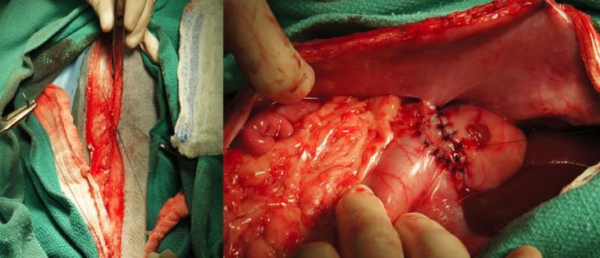
Although there are few differences between humans and veterinary patients, perhaps the most important similarity is the perception of physical and emotional distress and pain. There should be little doubt that reducing the degree of tissue injury in humans and animals will result in less pain and improve the quality of recovery for the patient. Laparoscopic cholecystectomy in humans has reduced the average hospital stay from 5 to 7 days to less than 24 hours and has resulted in significantly fewer complications including incisional failure and blood loss. Perhaps the most analogous procedural evolution in veterinary surgery is ovariectomy and the development of laparoscopic ovariectomy. Numerous studies have demonstrated less postoperative pain with few or no complications in dogs undergoing laparoscopic ovariectomy, which has made it the procedure of choice for many veterinarians. The same relationship exists for laparoscopic gastropexy (Figure 1) compared with open gastropexy (Figure 2). Because laparoscopy currently has the most applicability to general practice, the remainder of this article will discuss MIS as it relates to laparoscopy, specifically.
LAPAROSCOPIC INDICATIONS
At the current time, numerous indications for laparoscopy exist in veterinary medicine and surgery. The astute clinician would be wise to become comfortable with the ideas and principles of MIS as to provide refined surgical options to their clients. Minimally invasive surgery is not just for specialists. Rather, the most common procedures could be and are readily adaptable to general practice assuming the practitioner is dedicated to developing the skills necessary to become successful. Common indications for laparoscopy in general practice include ovariectomy (OVE), ovariohysterectomy (OHE), cryptorchidectomy, gastropexy, liver biopsy, pancreatic biopsy, lymph node biopsy, and intestinal biopsy. These procedures are being performed safely and effectively in many practices and the demand for them is increasing rapidly. Although there are geographic and demographic limitations this trend will continue into the future and will likely have significant economic consequences in veterinary practice.
LAPAROSCOPIC CONTRAINDICATIONS
A significant learning curve exists with performing laparoscopy. Well-developed psychomotor skills are a prerequisite but so is appropriate training. Many laboratories and courses are offered each year and should be attended if considering performing laparoscopy in practice. Thus, the first contraindication to MIS is inexperience or lack of comfort with procedures. Inexperienced or untrained staff is another contraindication, which is remedied by adequate training. Inadequate instrumentation is also a contraindication. When starting out, all laparoscopic procedures should be performed on an elective basis only. This will help to insure adequate planning and preparation so as to increase the chances of a successful outcome. Advanced procedures and procedures that require exploration of the abdomen are also not appropriate for the beginning endoscopist; traditional surgical approaches should be performed in these cases. One of the major limitations with traditional laparoscopy is the inability to feel or palpate organs. Instead, the laparoscopist relies on his or her ability to see and/or palpate with a probe the tissues of interest, which limits assess-ability.
LAPAROSCOPY EQUIPMENT
A variety of instruments are available and designed to be used with veterinary laparoscopy. A list and brief description of the more common instruments is included here:
- Camera: The camera is attached to the telescope and light source and is used to capture and transmit imaging from inside the abdomen to a video screen. There are two types of cameras used in veterinary endoscopy, 1-chip and 3-chip. In general, the 1-chip cameras have fewer pixels per unit area and reproduce color to a lesser degree than do 3-chip cameras. That being said, 1-chip cameras are significantly cheaper and produce images almost as bright and colorful as 3-chip cameras.
- Telescope: The telescope is a long rigid instrument, which attaches to the camera and is used to explore the peritoneal cavity. Typical telescopes are either 5 or 10 mm in diameter and either 0 or 30 degrees oblique. The most common scope in veterinary surgery is a 5 mm 0 degree.
- Light source: The light source most commonly used in veterinary surgery is xenon and is powered up to 300 Watts. The larger the wattage, the brighter the image.
- Insufflator: The insufflator is an automatic pump, which controls the flow rate and intra-abdominal pressure during the laparoscopic procedures. Carbon dioxide gas is used and is sourced from a high-pressure tank. Air is not used as it may result in air embolism.
- Cannula: A cannula or port is the instrument used to obtain and maintain access to the peritoneum. The cannula serves as a sleeve for the insertion and removal of the telescope and instruments.
- Trocar: Trocar refers to the combination of an obturator and cannula together.
- Obturator: The obturator is the inner component of the trocar and is either sharp or blunt. The obturator is removed once the trocar has been positioned correctly in the abdomen.
- Veress needle: A Veress needle is a small-gauge needle, which has an outer sharp edge and a spring-loaded, blunt inner obturator. It is used to penetrate the peritoneal cavity for insufflation prior to insertion of laparoscopic trocars.
- Surgical instruments: A variety of laparoscopic surgical instruments should be available:
- 5-mm blunt probe o 5-mm Babcock forceps
- 5-mm Clamshell biopsy forceps
- 5-mm Punch biopsy forceps
- 5-mm Kelly dissecting forceps
- 5-mm Metzenbaum scissors
- Bipolar Energy Devices: Either a LigaSure or Harmonic Scalpel should be included in a laparoscopy set. These are specialized instruments used for combined vessel/ tissue sealing and division. They are more effective at hemostasis and surgical efficiency compared with monopolar and earlier bipolar systems (e.g., Patton HotBlade). Both the LigaSure and Harmonic Scalpel systems come with a variety of hand pieces, which makes them incredibly versatile. The LigaSure is effective in sealing vessels <7 mm while the Harmonic Scalpel seals vessels <5 mm.
STERILIZATION
A number of different sterilization modalities are available. Typically, the scopes, cameras, light cables, and energy-based sealing devices are gas sterilized (e.g., ethylene oxide) as this improves instrument life. However, steam sterilizers can also be used for steel instruments. Most laparoscopic surgery instruments are composed of steel and can be sterilized in traditional steam sterilizers. Cold sterilization using 2% glutaraldehyde solution is also described for laparoscopic telescopes. The camera head can either be sterilized overnight in a gas sterilizer or can be reused by use of sterile sleeve covers. Because laparoscopic instruments tend to be made of small fragile components, careful cleaning practices are required to prevent damage and incomplete disinfection/sterilization.
CONCLUSION
In summary, MIS is an ever-evolving discipline that relates to most facets of surgery. Further, minimally invasive approaches are being requested with greater and greater frequency by animal caregivers just as they are by patients in human surgery. After all, human patients are frequently our clients and they often expect the same level of care for their pets. Minimally invasive veterinary surgery include many benefits such as less tissue trauma, less pain and quicker recovery are extremely desirable to our clients and the astute veterinarian would be wise to become familiar with these concepts and procedures so as to be able to offer the highest standard of care to his or her clients and patients. Many routine abdominal procedures can be and are currently being performed readily in general practice provided that the practitioner has invested in the appropriate equipment and training, and is committed to successfully performing routine procedures with regularity.